

Hysteria's Long Shadow
Psychological Factors in Multiple Autoimmune Syndrome


Some Background
This post is part of my lingering questions, asked and answered, in my research of Multiple autoimmune syndrome (when one person meets the study classification criteria for three or more autoimmune diseases). My question is based on a simple sentence from Cojocaru et. al’s 2010 article on Multiple autoimmune syndrome (MAS): “Familial or genetic, infectious, immunologic and psychological factors have been implicated in the development of MAS (1,2).” This article was my first introduction to the concept of Multiple autoimmune syndrome, and over the past several months, my posts have covered the twists and turns of the scientific evidence on this disease. Since I first reviewed it, I’ve noted that I wanted to find out more about “psychological factors” being “implicated in the development of MAS.” How come? Because when I hear anything that even remotely resembles a psychological cause for autoimmune symptoms, it makes me defensive. The New York Times, and others, have written more extensively on the concept of medical gaslighting:
I have also written about Diagnostic Power: that it is helpful to avoid an anxious appearance, if possible, when seeking evaluation for autoimmune symptoms, lest your symptoms be dismissed as anxiety-related hypochondria, or the fearsome M-word, malingerer (applied predominantly to women, and at one point, my young daughter). Should this advice be necessary? Emphatically No. Yet, here we are, in the year 2023.
Hysteria
4,000 years of mistaken thinking about women’s health, and its impact on current practice today, is searingly described by Elizabeth Land Quant, in her article, HYSTERIA & ME: AN ANCIENT, MISOGYNISTIC DISORDER IS KILLING WOMEN. In the article she describes how she was mistakenly diagnosed with fibromyalgia and related psychological disorders, causing maltreated disability for several years. Due to her persistence, she was eventually diagnosed with a different disorder that, unlike fibromyalgia, has a definitive and available test, and has an effective treatment regimen. Because of the delay in accurate diagnosis and treatment, she suffered permanent, untreatable, damage to her body. She notes:
The problem is not that doctors identify mental health disorders as one potential cause of physical symptoms. The problem is that those same physical symptoms could also be caused by a number of physical diseases. This is the point where the effective process of a proper diagnosis breaks down. Instead of testing and ruling out physical disease, many doctors jump to the assumption of the absence of physical disease. Having a mental illness does not make us immune to having a physical disease.
Seventy-five percent of Americans with autoimmune disease are women, according to the American Autoimmune Related Disease Association and it takes on average three years and four doctors to get a diagnosis of an autoimmune disease. The study “Frequency of Symptoms of Ovarian Cancer in Women Presenting to Primary Care Clinics” shows that even though 89% of women with early stages of ovarian cancer have a distinct set of symptoms (bloating, abdominal pain, urinary symptoms, fatigue, back pain, constipation) that they report to a doctor, “only 20% percent of cases are caught in an early stage.” How many of these women were dismissed by their doctors because their symptoms fit a somatic illness or were written off as general reproductive issues that halted further testing?
The whole article is well worth reading. Unfortunately, the author’s personal experience is all too common among autoimmune disease symptom sufferers. To offer a countervailing point to misogyny, doctors are trained and financially incentivized to offer the most common explanations to a problem (the science on what is common depends on what you’re looking for, of course), and to offer the least amount of testing possible to arrive at the most likely diagnosis—unconscious bias affects every inch of this process. Physicians have the expectation that if symptoms continue or worsen, the person will return to them for further assessment and work up. This ignores the complex barriers that exist for the vast majority of patients seeking care—when even those with financial resources and good health insurance are likely to encounter barriers with getting time off work and/or finding alternative childcare arrangements, or interpret their physician’s conservative assessment as a dismissal of symptoms. Hysteria and women’s health could be, and probably already are, a substack newsletter in and of themselves, so I’ll leave it here and return to the topic at hand.
What are the psychological factors in Multiple autoimmune syndrome?
I read the two references cited by Cojocaru et. al. and discovered…crickets. There was nothing in the text of either reference about psychological factors implicated in Multiple autoimmune syndrome. But, I still had some questions that compelled me to research further. After all, psychological disorders and autoimmune disease can be linked, right? We need look no further than psychosis associated with thyrotoxic storm in Graves disease. And, at some point in the past, from a reference I failed to record, I read or heard that schizophrenia had an autoimmune association. If true, this connection is personally relevant to me because I had a Great Uncle with Schizophrenia, which may provide yet more evidence of autoimmunity in my family. To the science!
Autoimmune Diseases and Psychotic Disorders is a 2019 Danish review of the scientific evidence to date, including meta-analyses. According to the authors, Schizophrenia has been hypothesized to be related to an autoimmune process since the 1930s. In the ‘50s and ‘60s, a co-occurrence of Celiac disease and Schizophrenia was observed. Autoantibodies that reacted with brain antigens were discovered in Schizophrenic patients around mid-century as well, but could not be determined to be causative. In their review, as this chart shows, the scientific picture is decidedly mixed.
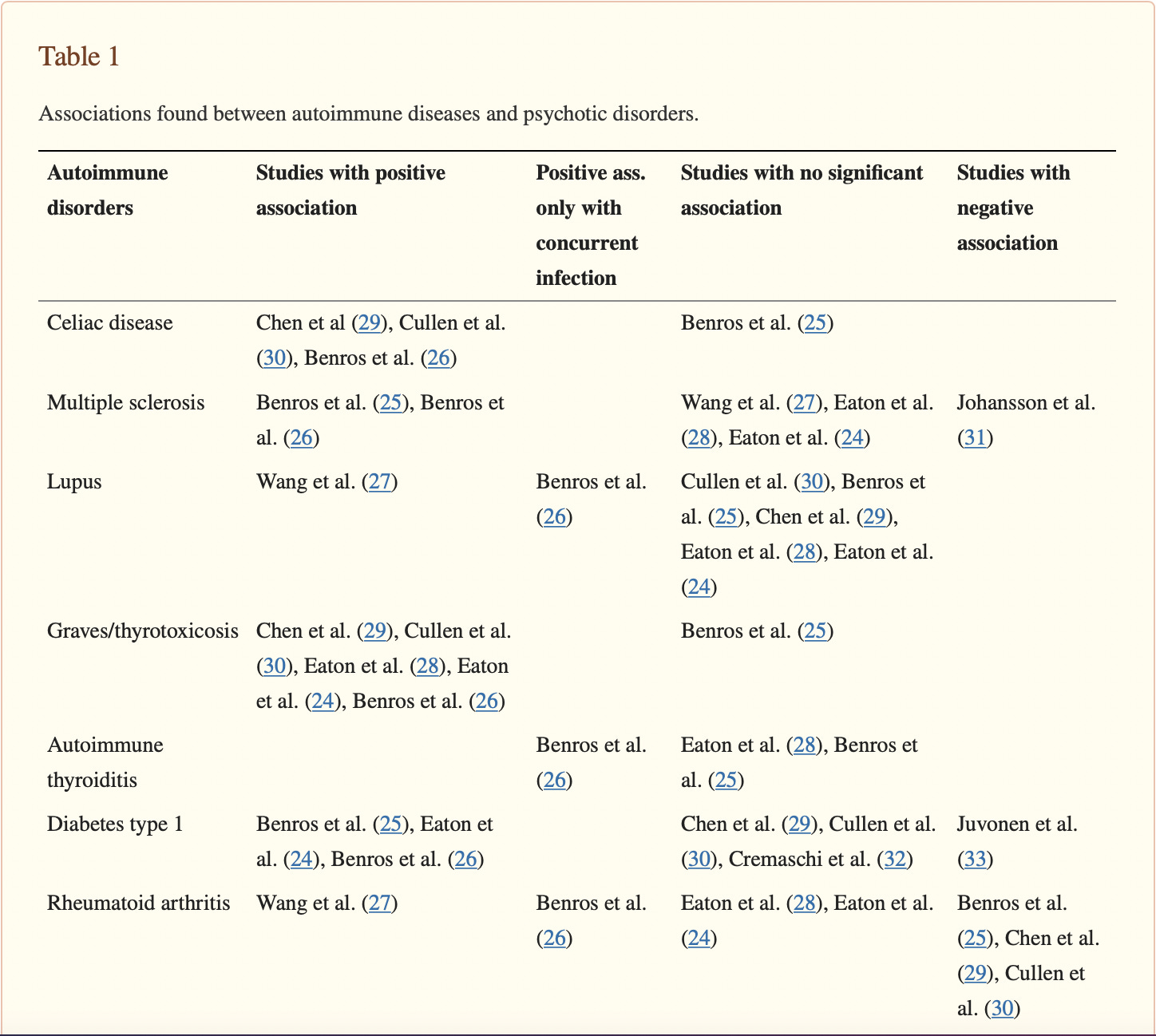


(Jeppesen & Benors, 2019)
The authors note that when schizophrenia is the presenting diagnosis, underlying autoimmune disease may be overlooked. This strikes me as a spectacular understatement, considering how difficult it is for patients who are not actively psychotic to receive a comprehensive work up for autoimmune disease. It’s easy to imagine how difficult it would be for someone with psychosis to effectively communicate their symptoms to get a physician to look past their psychosis and take notice of autoimmune symptoms.
The authors report that the evidence, on balance, appears to support an association between psychosis and Celiac disease, Multiple sclerosis, Lupus and Autoimmune thyroid disease. There is not enough evidence to claim an association between psychosis and other autoimmune diseases, although such associations cannot be ruled out. The authors go on to recommend:
Focus on the association between autoimmunity and psychosis, regardless of etiology, is important, not only for researchers but also for the individual patient. It is known that patients suffering from schizophrenia have an excess early mortality, with a life expectancy up to 13.5 years shorter than the general population, primarily due to physical diseases (122). Bearing this in mind and considering that patients with psychotic disorders might struggle with reporting on somatic symptoms, it is important for clinicians to be aware of an increased prevalence of autoimmune disease in this group. Symptoms from a disease such as celiac disease or rheumatoid arthritis might very well be overlooked and cast aside as a part of the patient's psychosis, or possibly adverse events caused by their treatment. With increasingly sufficient treatment strategies in autoimmune diseases, overlooking and therefore not treating these diseases, increases the health gap between those with schizophrenia and the general population even further. Therefore, patients with a psychotic disorder need to be thoroughly and frequently examined when presenting with symptoms possibly related to autoimmunity or other health problems.
(Jeppesen & Benors, 2019)
And here’s where the intersection of Hysteria, psychosis and autoimmunity gets really thorny for me. I want people suffering from Schizophrenia or psychosis to receive comprehensive diagnostic work up and treatment for other diseases that they might have, and which may legitimately improve their psychotic symptoms, without psychosis being erroneously diagnosed in people who primarily need to be diagnosed and treated for autoimmune disease. The distance between what researchers are recommending and what is happening in clinical practice is disappointingly vast.
References
Cojocaru M, Cojocaru IM, Silosi I. Multiple autoimmune syndrome. Maedica (Bucur). 2010 Apr;5(2):132-4. PMID: 21977137; PMCID: PMC3150011.
Jeppesen R, Benros ME. Autoimmune Diseases and Psychotic Disorders. Front Psychiatry. 2019 Mar 20;10:131. doi: 10.3389/fpsyt.2019.00131. PMID: 30949074; PMCID: PMC6435494.
Sloka S. Observations on recent studies showing increased co-occurrence of autoimmune diseases. J Autoimmun. 2002;18(3):251–257.[PubMed] [Google Scholar] [Ref list]
Wielosz E, Majdan M, Zychowska I, et al. Coexistence of five autoimmune diseases: diagnostic and therapeutic difficulties. Rheumatol Int. 2008;28(9):919–923. [PubMed] [Google Scholar] [Ref list]