

If a joint hurts at home, and no one's (doctor's) around to see it, does it make a sound?
If a joint hurts at home, and no one's (doctor's) around to see it, does it make a sound?
Palindromic Rheumatism and its diagnostic problems


The answer to the title question is no. Why? Because if a physician does not witness the joint inflammation, then any of four proposed diagnostic criteria for Palindromic rheumatism has not been met. Yes, you read that right, there are four proposed diagnostic criteria, with no consensus criteria, for Palindromic rheumatism. For an arthritis that is characterized by it’s unpredictable onset, short duration, and lack of detectable, residual joint damage, it’s easy to see the difficulty in getting a diagnosis. For preliminary descriptive information on Palindromic rheumatism, please check out my work-in-progress Diagnosis Description here. I include the four proposed diagnostic criteria below, for reference. I have not yet found that any of the proposed criteria has been scientifically validated.
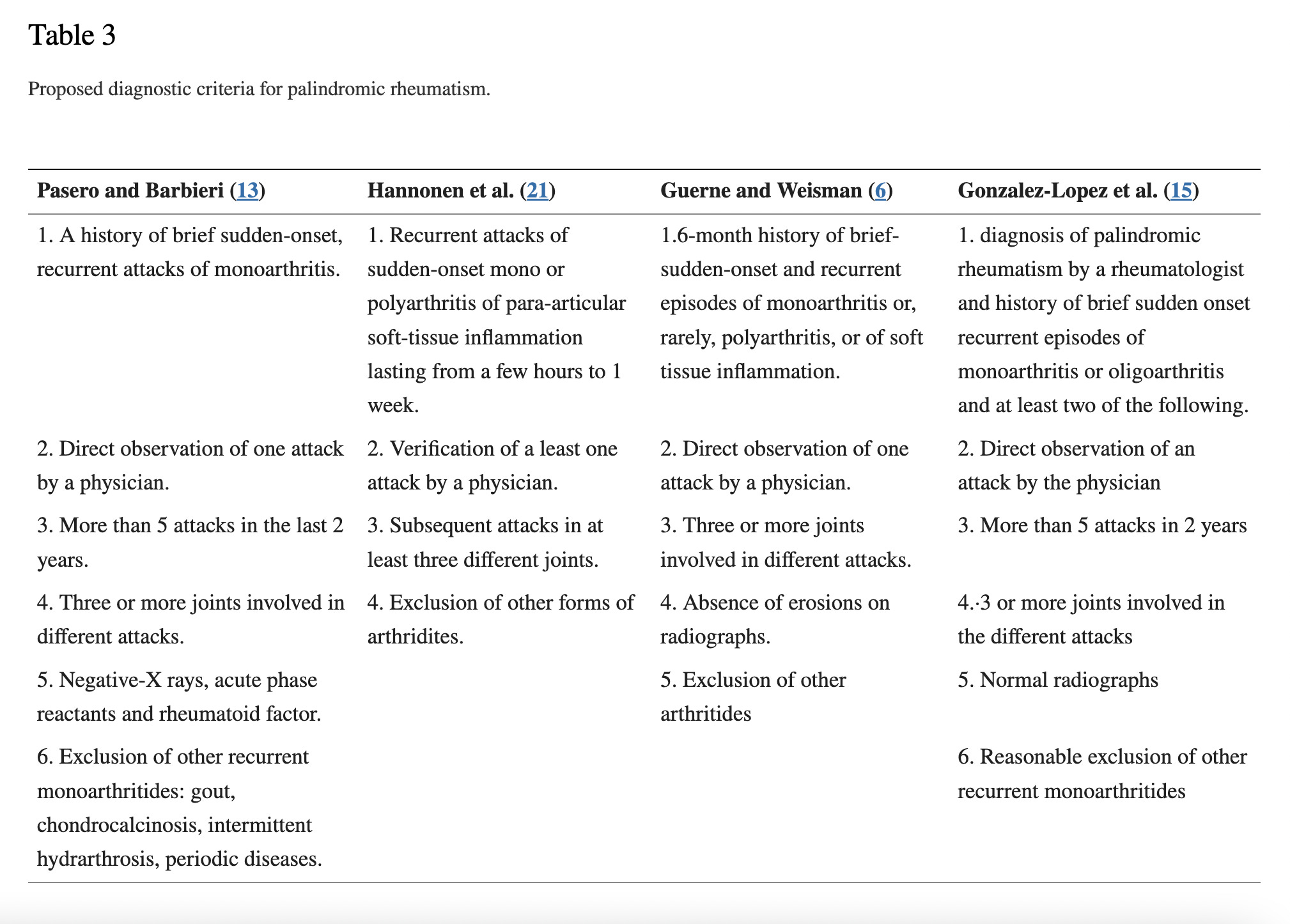
(Sanmartí et. al, 2021)
My definitions of Table 3 terms: monoarthritis = arthritis in one joint; acute phase reactants = components of the innate (immediate) immune response, such as cytokines (molecules that exert a pro- or anti-inflammatory effect); monoarthritides = all other types of arthritis that affect one joint; chondrocalcinosis = the calcification (hardening) of joint cartilage; hydrarthrosis = excess synovial (a gel-filled capsule between two bones) gel causes inflammation and swelling in a movable joint; para-articular = around a joint; erosions = damage to bone; arthritides = all other types of arthritis; oligoarthritis = 2-4 joints are inflamed.
First witnessed by a Mayo Clinic physician (Hench) in 1928, then
34 similar cases were followed and reported on by Hench, and his colleague, Rosenberg. Their report, in which they coined the name “Palindromic rheumatism,” was published in 1944. As someone who loves language, I was hoping for a detailed analysis of how the signs and symptoms of this disease are the same backwards and forwards, like a palindrome. No such luck. The term is an artifact from ancient Greece, used by Hippocrates to name other diseases that come and go. Sanmarti et. al, note a quote in their review article that makes plain that, even at the time, the authors were defensive about the accuracy of the name. Something along the lines of, what’s good enough for Hippocrates is good enough for you. Meh, not really guys.
(Sanmartí et. al, 2021)
Circling back to the proposed diagnostic criteria: hydrarthrosis is an exclusion criteria?
That means that anyone with inflammation of the synovium (a.k.a. hydrarthrosis) cannot be diagnosed with Palindromic rheumatism. (The synovium is like a gel pack nestled between two bones to cushion a joint. Some joints in the body are synovial joints, such as joints in the knees, wrists and hands. A few joints in the body are not synovial joints, such as rib joints and the front pelvic joint (symphysis pubis).) Excluding synovial inflammation from the diagnosis of Palindromic rheumatism is critical to understanding the controversies surrounding this under-studied collection of signs and symptoms.
The Controversies
Palindromic rheumatism precedes Rheumatoid arthritis (with characteristic synovial joint inflammation)
Palindromic rheumatism could be a distinct manifestation of an inherited autoinflammatory disease coded by variations in the familial Mediterranean fever gene (a.k.a. gene MEFV)
Palindromic rheumatism precedes other autoimmune diseases (with characteristic synovial joint inflammation)
1. Palindromic rheumatism precedes Rheumatoid arthritis (with characteristic synovial joint inflammation)
A 2019 Canadian study of 154 participants with early rheumatoid arthritis (ERA) found that 42% “reported a history of episodic joint pain and swelling, half of whom reported that these symptoms preceded ERA diagnosis by over 6 months” (Ellingwood et. al, 2019).
Depending on study classification criteria, participants with a diagnosis of Palindromic rheumatism progress to Rheumatoid arthritis anywhere from 10-66% of the time (Sanmartí et. al, 2021). 10-66% is a huge scientific spread reflecting the lack of consensus around study classification and diagnostic criteria, which confounds the collection of comparable results.
A 2020 study found that out of 158 participants with Rheumatoid arthritis, 18% had a pre-recorded diagnosis of Palindromic rheumatism. In those 29 participants, the median duration of disease progression from Palindromic rheumatism to Rheumatoid arthritis was 1.2 years. (Castellanos-Moreira et. al, 2020)
2. Palindromic rheumatism could be a distinct manifestation of an inherited autoinflammatory disease coded by the familial Mediterranean fever gene (a.k.a. gene MEFV)
An interesting 2021 Spanish study of 76 participants with “Palindromic-like arthritis”, was able to classify participants into four categories based on antibody testing and gene analysis. Their inclusion criteria for Palindromic-like arthritis was very broad, defined as “predominantly short attacks (≤ 7 days) and a relapsing course.” (Cuervo et. al, 2021). Relapse means that the same symptoms happen again. (I’m just now realizing that three out of the four articles I reference include the author of the case study and review article I have been quoting most frequently—Sanmarti—which gives me additional confidence in the accuracy of the review article.) But back to the four categories found in this observational retrospective study:
15 of the 76 participants with Palindromic-like arthritis carried Mediterranean fever gene variations. 9 out of 15 participants with Mediterranean fever gene variations did not meet the criteria for a Familial Mediterranean Fever diagnosis, suggesting that Palindromic rheumatism is a distinct manifestation of Familial Mediterranean Fever gene variations.
21 of the 76 participants had rheumatoid factor (RF) and/or anti-citrullinated protein antibodies (ACPA) autoantibodies. 10 of the 21 participants with autoantibodies later met the American College of Rheumatology/European League Against Rheumatism classification criteria for Rheumatoid arthritis after several years of follow up. Some, who met the criteria for Rheumatoid arthritis, developed bone-damaging disease.
35 of the 76 participants had neither Mediterranean fever gene variations, nor autoantibodies.
5 of the 76 participants had Mediterranean fever gene variations and a previously diagnosed autoimmune disease, which was deemed to be in remission.
(Cuervo et. al, 2021)
The findings of this study are important because almost half of participants had a genetic variation or autoantibody as a potentially causative factor for symptoms. This study was a retrospective observational study, so the potential that hidden bias affected results is high, but as a jumping off point for additional research, this study is important.
3. Palindromic rheumatism precedes other autoimmune diseases (with characteristic synovial joint inflammation)
There is outdated evidence to suggest that after an initial diagnosis of Palindromic rheumatism, patients later come to meet the criteria for other autoimmune diseases, including Sjogren’s syndrome, Psoriatic arthritis, Vasculitis, Myositis, Behcet’s disease, and Systemic lupus erythematosus. The evidence-based associations with the autoimmune diseases listed are much lower than the association between Palindromic rheumatism and Rheumatoid arthritis. (Sanmartí et. al, 2021)
Why it Matters
Palindromic rheumatism could be the canary in the coal mine for Rheumatoid arthritis, Mediterranean fever gene variations, or other rheumatological autoimmune disease. It has the potential to be an early prompt for comprehensive work up to determine type of underlying cause, and identify early treatment. Early treatment that is targeted based on autoantibody profile or genetic variation could prevent progression to better-defined autoimmune diseases and/or permanent tissue damage in some patients. The challenge is in recognition, both by the person experiencing signs and symptoms, and the clinician evaluating them. What can you do if you’re experiencing symptoms? Excellent time- and date-stamped photo-documentation of affected joint(s), which can be accomplished on most cell phones. Accompany the photos with comprehensive journal entries that include when symptoms started, how symptoms felt (aching, stabbing, prickling, throbbing), how long symptoms lasted (hours, days, weeks), signs of inflammation (redness, rash, swelling, hot skin), actions that make symptoms start or worsen (examples: medicine, exercise, trauma, stress, diet), and actions that make symptoms better or resolve (examples: heat/ice, medicine, rest, diet).
Next week’s post will address the scientific research on Palindromic rheumatism in greater detail.
References
Castellanos-Moreira R, Rodriguez-Garcia SC, Gómez-Puerta JA, Ruiz-Esquide V, Camacho O, Ramírez J, Cuervo A, Morlà R, Cañete JD, Haro I, Sanmarti R. Rheumatoid Arthritis Initiating as Palindromic Rheumatism: A Distinct Clinical Phenotype? J Rheumatol. 2020 May 1;47(5):652-657. doi: 10.3899/jrheum.190061. Epub 2019 Aug 1. PMID: 31371648.
Cuervo A, Sanmartí R, Ramírez J, Castellanos-Moreira R, Inciarte-Mundo J, Aróstegui JI, McGonagle D, Cañete JD. Palindromic rheumatism: Evidence of four subtypes of palindromic-like arthritis based in either MEFV or rheumatoid factor/ACPA status. Joint Bone Spine. 2021 Dec;88(6):105235. doi: 10.1016/j.jbspin.2021.105235. Epub 2021 Jun 5. PMID: 34098104.
Ellingwood L, Schieir O, Valois MF, Bartlett SJ, Bessette L, Boire G, Hazlewood G, Hitchon C, Keystone EC, Tin D, Thorne C, Bykerk VP, Pope JE; CATCH Investigators. Palindromic Rheumatism Frequently Precedes Early Rheumatoid Arthritis: Results From an Incident Cohort. ACR Open Rheumatol. 2019 Oct 21;1(10):614-619. doi: 10.1002/acr2.11086. PMID: 31872182; PMCID: PMC6917323.
Sanmartí R, Frade-Sosa B, Morlà R, Castellanos-Moreira R, Cabrera-Villalba S, Ramirez J, Salvador G, Haro I, Cañete JD. Palindromic Rheumatism: Just a Pre-rheumatoid Stage or Something Else? Front Med (Lausanne). 2021 Mar 25;8:657983. doi: 10.3389/fmed.2021.657983. PMID: 33842513; PMCID: PMC8026891.