

Primary care diagnosis and management of Polymyalgia rheumatica: an autoimmune disease anomaly
Primary care diagnosis and management of Polymyalgia rheumatica: an autoimmune disease anomaly

Every time I think I’m on solid ground, as I did with Polymyalgia rheumatica, the ground starts to shift when I take a deeper dive.
What I Thought Was Solid Ground
As a nurse working in primary care—also known as your internist’s, general practitioner’s, family medicine doctor’s, adult medicine doctor’s office—there were a lot of patients with co-occurring autoimmune diseases that complicated the conditions their primary care physician treated. There were not a lot of autoimmune diseases the primary care physicians diagnosed or treated themselves. Usually the primary care physician would conduct some preliminary testing and based on those results, refer suspected autoimmune cases out to a specialist (rheumatology, neurology, gastroenterology), etc. The exception to this rule was Polymyalgia rheumatica and, sometimes, Hashimoto’s thyroiditis. The physician I worked with had a standard workup regimen and treatment protocol for Polymyalgia rheumatica. At the time, it didn’t even occur to me to ask questions about the anomaly of a primary care physician diagnosing and treating Polymyalgia rheumatica alone, out of all of the autoimmune diseases that exist. But this week, it’s a question I can’t get out of my mind.
If you have an autoimmune condition that can be diagnosed and treated by your primary care physician, the benefits are clear: no hurdles to leap to get a referral, shorter wait times for appointments, likely lower costs. Your primary care provider is the closest you come to a physician who sees your full medical picture and treats you as whole, interconnected person, rather than a collection of parts. All of these factors combine to create greater access to care. There must be something fundamental to the diagnosis of Polymyalgia rheumatica that anchors it more firmly to definitive diagnosis and treatment. What are those fundamental qualities, and how can they be compared to other autoimmune diseases as an example of effective diagnosis?
It Still Has Multiple Criteria, Putting It On Shaky Ground
There are several different classification or diagnostic criteria for Polymyalgia rheumatica. The American College of Rheumatology and the European League Against Rheumatism published provisional classification criteria in 2012. This was after several years of study, international rheumatologist surveys, and consensus building. And it’s still just provisional classification criteria. I don’t know enough yet to know whether the 2012 criteria is what is being primarily used to study Polymyalgia rheumatica, but that’s something I’ll be looking at in the coming week.
This 2019 Swedish study researches the diagnosis of polymyalgia rheumatica in primary care, using the five criteria that exist to test the validity of a primary care diagnosis. Here are the five criteria:

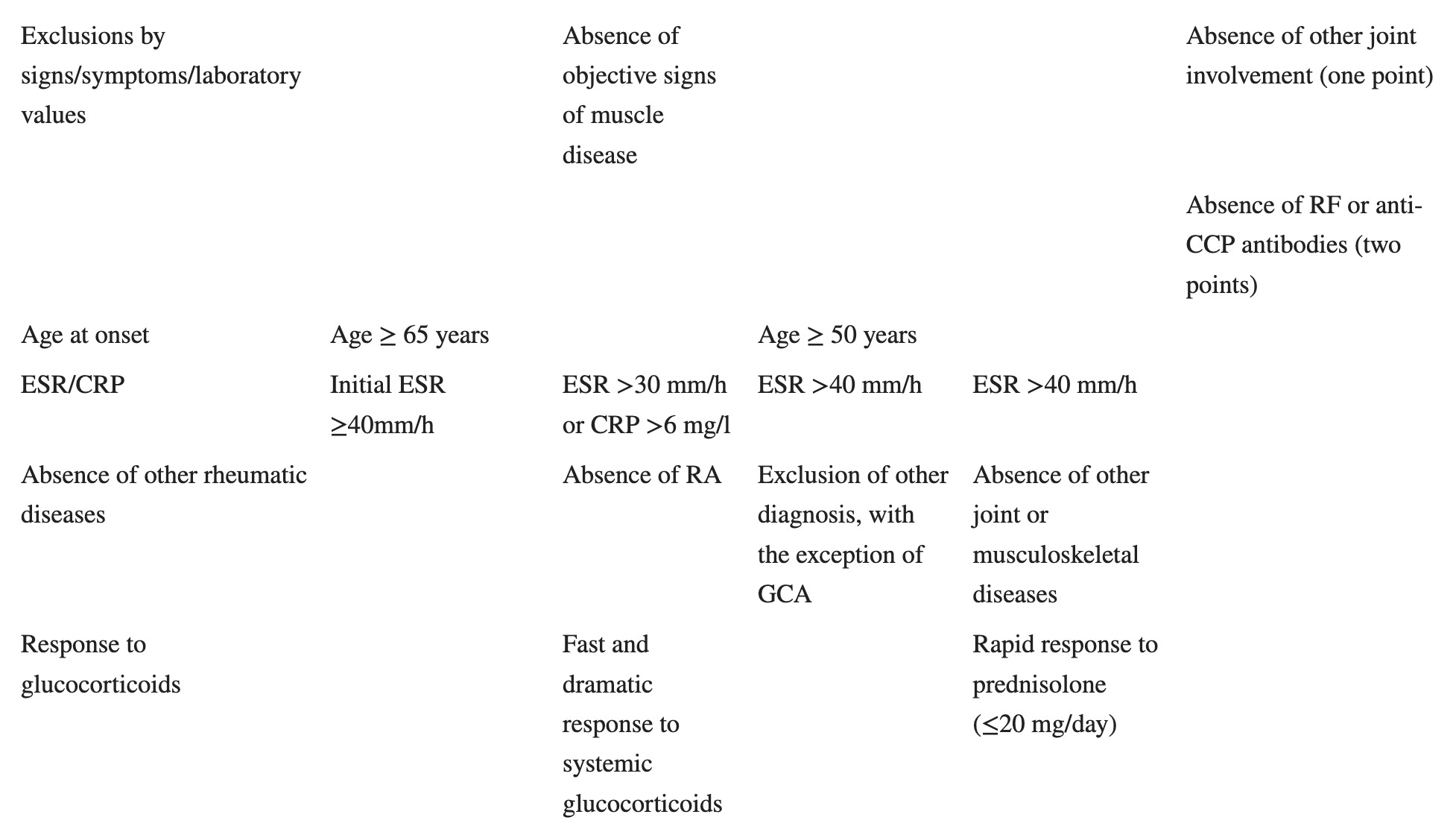
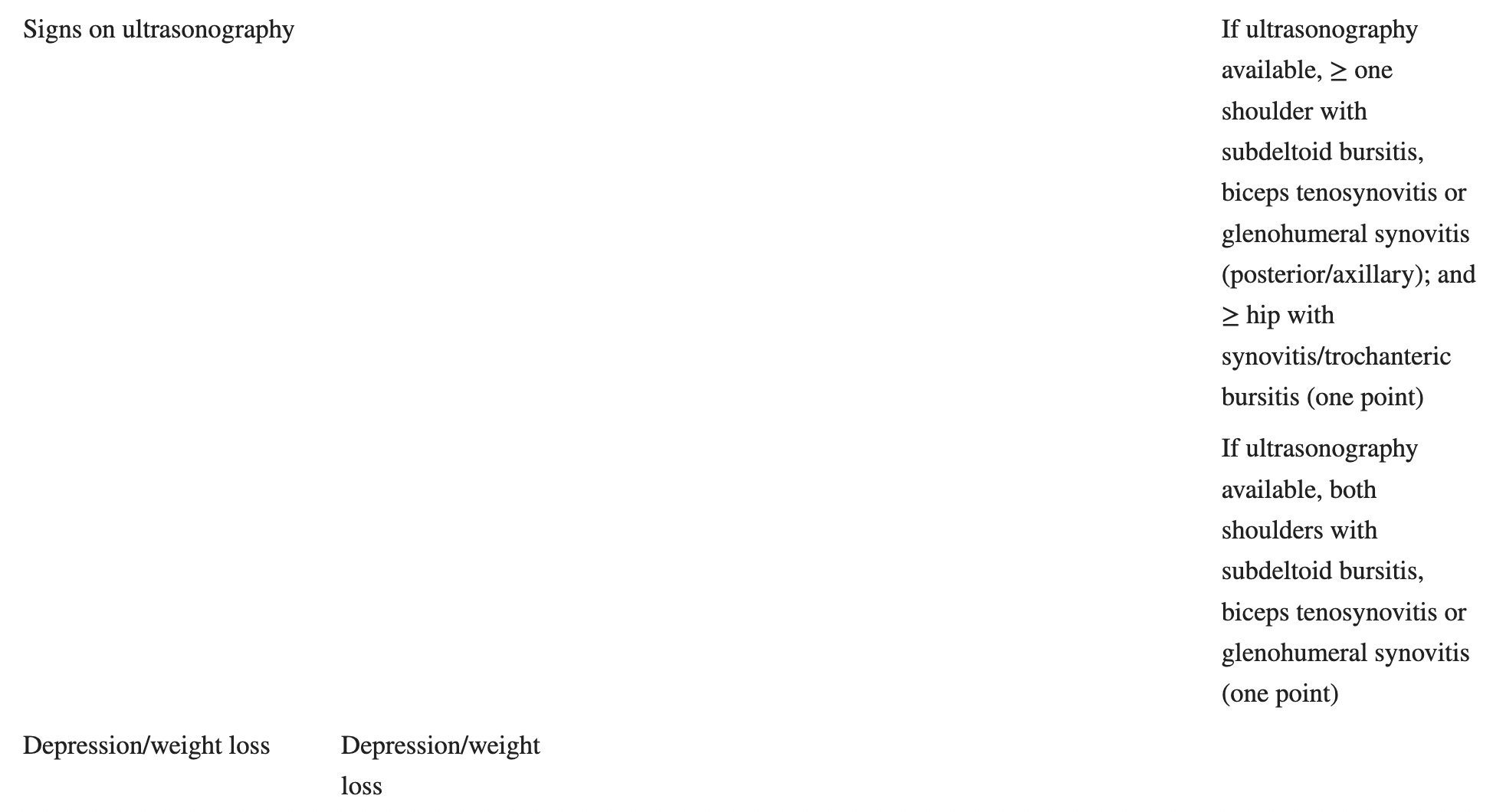
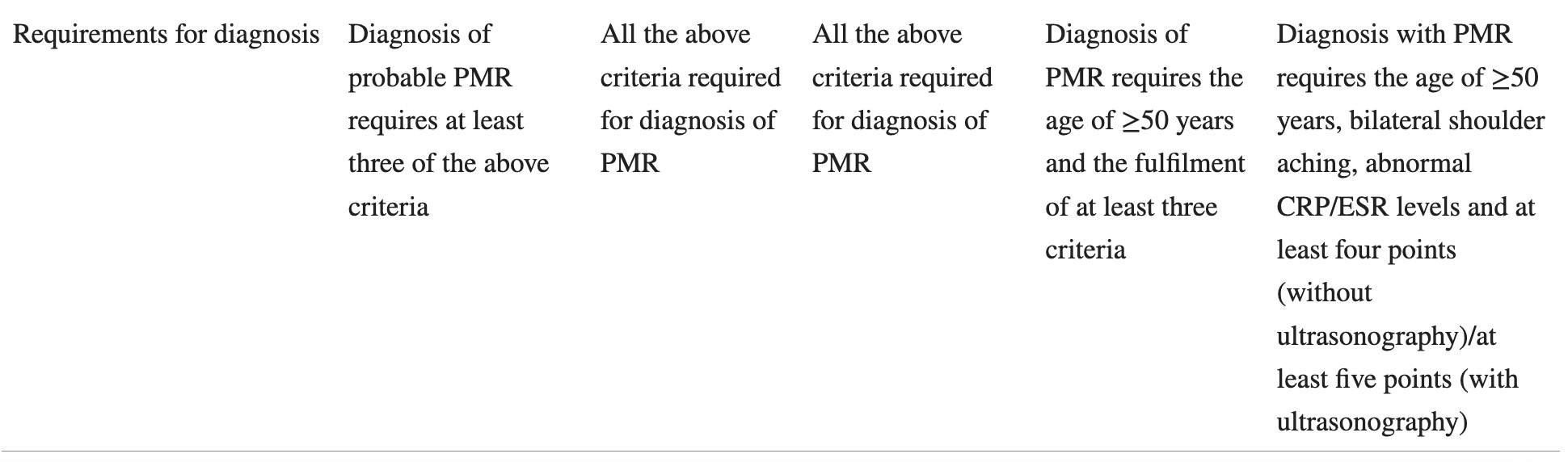
(Fors et. al, 2019)
The Fors study found that out of all the criteria, the 2012 criteria was the most consistent with patients diagnosed with Polymyalgia rheumatica in primary care. Most of the patient cohort studied received a diagnosis of Polymyalgia rheumatica prior to the publication of the provisional 2012 criteria, countering the criticism that the majority of patients validated the 2012 criteria because the 2012 criteria was used to diagnose them.
It’s Common, With a Standard Treatment
This American College of Rheumatology quote points to the reason Polymyalgia rheumatica is so often diagnosed and treated in primary care:
Polymyalgia rheumatica (PMR) is a common inflammatory rheumatic disease of older individuals and a common indication for long-term corticosteroid therapy.
This editorial article posted on the American College of Rheumatology’s website comments on the provisional nature of the 2012 criteria and discusses why Polymyalgia rheumatica is most commonly diagnosed and treated in primary care:
It is important to emphasize that these proposed criteria are provisional (meaning that they must ultimately be confirmed in additional prospective validation cohorts) and not diagnostic criteria. Classification criteria are useful for defining patient groups for clinical or epidemiologic studies. They are not developed or intended to define diagnoses in clinical practice. This point seems particularly relevant in PMR, a syndrome that is common, eminently treatable, and most often initially encountered by and treated by primary care providers rather than rheumatologists.
Great! Common, Recognizable and Treatable. Except…
The Provisional 2012 classification criteria note that the problem with the diagnosis and treatment of Polymyalgia rheumatica is in differentiating it from other autoimmune diseases (emphasis in bold is mine):
Difficulties in diagnosing and classifying patients with PMR are inherent in its definitions (9,10). The proximal pain and stiffness syndrome can occur at presentation in many other rheumatologic inflammatory illnesses in older people (1,2,7,9). Approximately half of patients diagnosed with PMR may have distal manifestations such as peripheral arthritis, hand swelling with pitting edema, and carpal tunnel syndrome (1,2,7,11). Polymyalgic presentation is common in late-onset rheumatoid arthritis (RA) and spondylarthritis and is also associated with giant cell arteritis in 10–30% of cases (1,2). Heterogeneity in the disease course, uncertainty regarding disease assessment parameters, and evolution of alternative diagnoses on followup complicate the management of PMR (9,12–15). For the above reasons a safe and specific approach preferring a relative underdiagnosis to an overdiagnosis is needed in PMR (9,11).
Thud. Preferring a relative underdiagnosis to an overdiagnosis means weighting the scales toward under-treatment. I can’t help but see the human cost in that: confused and frustrated people without a diagnosis, and in a lot of pain. Reassuringly, the editorial article, elevated by the American College of Rheumatology, addresses this issue for clinicians:
Is the sensitivity of these criteria adequate for practicing clinicians, recognizing that if the criteria are adopted, a third of patients they confront with PMR would be doomed to unnecessary suffering, when low-dose corticosteroids could rapidly ameliorate their often agonizing pain? Although the authors indicate the dangers of overdiagnosis of this condition because of the potential of overusing corticosteroids, when used judiciously in relatively low doses with appropriate attention to the management of comorbidities, this therapy can have a very favorable risk–benefit profile (4).
Functionally, this leads to the common practice of treating to diagnose. If your primary care physician suspects Polymyalgia rheumatica, treats you with corticosteroids, and you don’t experience remission of symptoms, then you don’t have Polymyalgia rheumatica. You must have something else. Sort of, probably. Time for that rheumatology referral.
Next week, there’ll be more on Polymyalgia rheumatica, specifically what is known about its particular disease mechanisms. For those who are new to AutoimmuneDx, I am currently writing posts based on reader-requests for more information and analysis on particular autoimmune diagnoses. If you would like me to take a closer look at a particular diagnosis, please leave a comment below. If you don’t feel comfortable commenting publicly, email me at autoimmunedx@gmail.com.
References
Fors C, Bergström U, Willim M, Pilman E, Turesson C. Validity of polymyalgia rheumatica diagnoses and classification criteria in primary health care. Rheumatol Adv Pract. 2019 Aug 27;3(2):rkz033. doi: 10.1093/rap/rkz033. PMID: 31660474; PMCID: PMC6799851.