


Whole Exome Sequencing
in Multiple Autoimmune Syndrome and Sjogren's Syndrome


They did it! Johar et al (including Anaya) studied molecular genetic analysis in multiple autoimmune syndrome, just as they roadmapped in Anaya’s 2014 publication The diagnosis and clinical significance of polyautoimmunity and Johar et al’s March 2015 publication Candidate gene discovery in autoimmunity by using extreme phenotypes, next generation sequencing and whole exome capture. (Multiple autoimmune syndrome is a condition where one person meets the diagnostic criteria for three or more autoimmune diseases.)
Their June 2015 study results include a tiny sample size—just 12 people—so their results are limited, but truly revelatory. If I sound breathlessly excited, then I’m accurately conveying my reaction to this study. Scientists, doctors and journalists, in their pretense of objectivity, don’t get to sound breathlessly excited. Who does? This lady.
Why am I breathlessly excited about this study?
Novel and rare functional genomic variants in multiple autoimmune syndrome and Sjögren’s syndrome is an observational retrospective study that includes study participants recruited because of their diagnosis of multiple autoimmune syndrome and Sjogren’s syndrome, as well as a control group. It is the control group that makes this study retrospective, and less susceptible to hidden bias than a cross-sectional study, but more susceptible to bias than a prospective study or clinical trial. The study uses whole exome sequencing, a type of genetic analysis that is
A laboratory process that is used to determine the nucleotide sequence primarily of the exonic (or protein-coding) regions of an individual’s genome and related sequences, representing approximately 1% of the complete DNA sequence. Also called WES and WXS” (National Cancer Institute, 2022).
Johar et al. further explain that
Whole exome sequencing (WES) is a widely used strategy for detection of protein coding and splicing variants associated with inherited diseases.
Whole exome sequencing is cost-effective, and focuses on areas of the genome where variations are likely to cause disease (Johar et al., June 2015).
This study used whole exome sequencing to test eight patients with multiple autoimmune syndrome (all eight were first diagnosed with Sjogren’s syndrome), four patients diagnosed with Sjogren’s syndrome alone, and 38 unaffected individuals. The exome sequences of the study participants were compared to two exome sequence databases: the Single Nucleotide Polymorphism database (dbSNP) and the 1000 Genomes Project. The Single Nucleotide Polymorphism database has since been subsumed by the database of Genotypes and Phenotypes (dbGaP). The database comparison is important because it expands the study’s exome comparison from 38 unaffected individuals to thousands of exome sequences. Five separate data filtering tools were used to identify “potentially damaging” genetic variations. If one of those five tools identified the variation as potentially damaging, then that variation was included in the results.
In 10 out of 12 of the study participants, 11 variants in the following genes were identified as potentially damaging: DUSP12, GRIN3B, KIAA0754, MACF1, LRP1, STAT6, BABAM1, ANKLE1, TMEM161A, MICAL1, ICA1, FKRP and CELA1.
Did your eyes just skim over that acronym buffet? Mine did, too.
First things first: the simple math. 11 variants in 13 genes in 10 out of 12 patients with exome variations?
the gene, dual specificity phosphatase 12 (DUSP12), has one never-before-found variant
the gene, GRIN3B, has one never-before-found variant
the genes KIAA0754 and MACF1 share one rare variant that affects them both
the gene, MACF1, has one additional, never-before-found variant that it doesn’t share with any other gene
the genes low density lipoprotein receptor-related protein 1 (LRP1) and signal transducer and activator of transcription 6 (STAT6) share one never-before-found variant that affects them both
the genes BABAM1 and ANKLE1 share one never-before-found variant that affects them both
the gene, transmembrane protein 161A (TMEM161A), has one never-before-found variant
the gene, microtubule-actin crosslinking factor 1 (MICA1), has one never-before-found variant
the gene, islet cell autoantigen 1 (ICA1), has one never-before-found variant
the gene, FKRP, has one never-before found variant
the gene, chymotrypsin-like elastase family, member 1 (CELA1), has one rare variant
That’s a total of 11 variants in 13 genes, two of which are rare when compared to the two large exome database comparisons. 9 of the variants are completely new to science at the time of publication.
To create a more visual representation of the study’s findings, I created the graphic below based on the authors results.
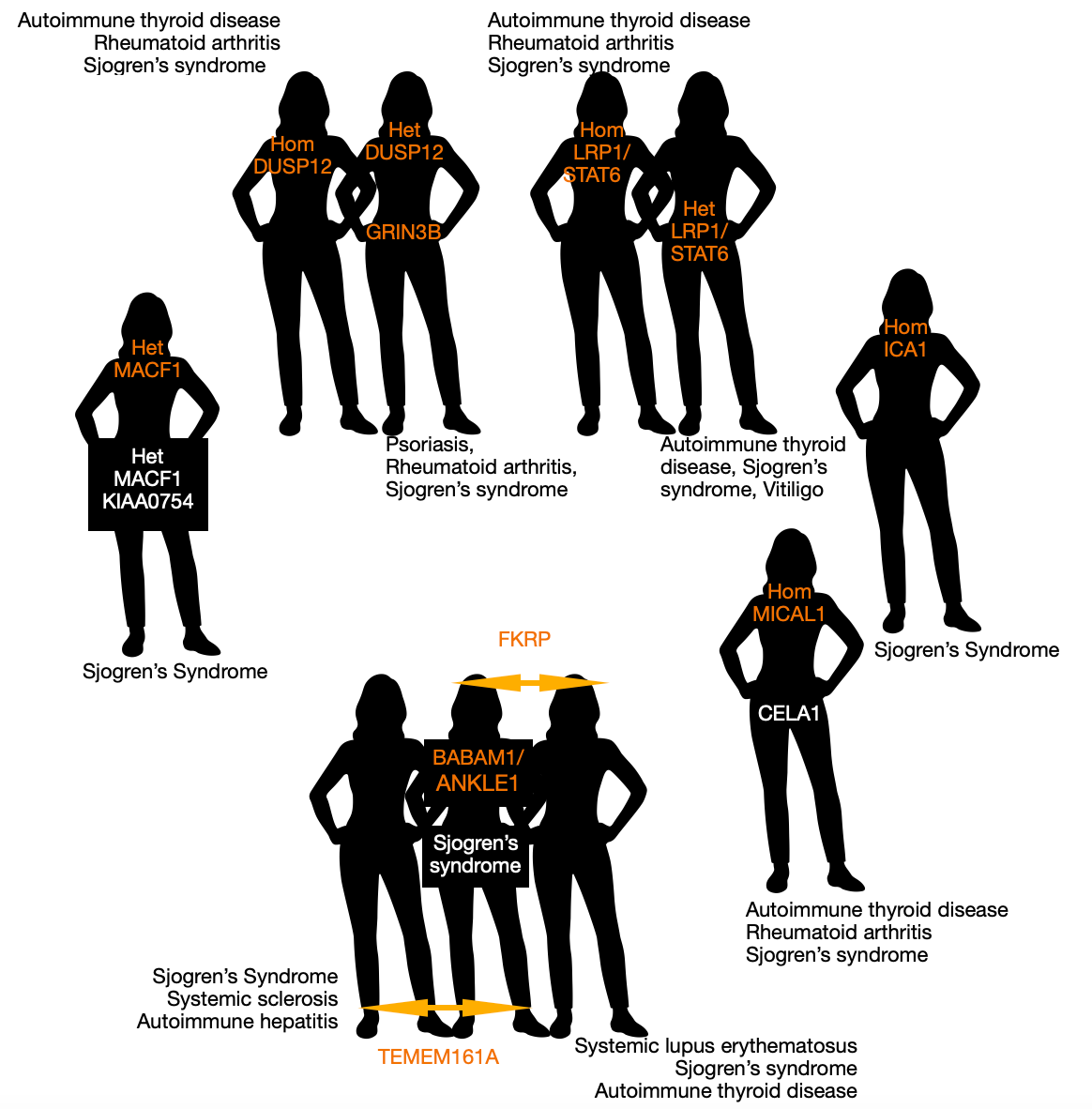
(Hom = homozygous. Het = heterozygous. Genes in orange are never-before-found variants in study participants. Genes in white are rare variants in study participants.)
What is astonishing to me is that out of an incredibly small study population—just 12 people—two separate pairs of study participants, that you can see at the top of the pictogram, both share new-to-science variants. The trio of participants at the bottom is also fascinating. The middle study participant was found to have three novel variants that are potentially damaging, one of which is unique to her (on gene BABAM1/ANKLE1), but the other two variants are each shared with one other study participant, shown standing on either side of her (Left: a variant on gene TEMEM161A. Right: a variant on gene FKRP). It’s interesting to me that with three novel variants, this central participant of the trio, was one of the study participants diagnosed only with Sjogren’s syndrome, while the participants who flank her both have multiple autoimmune syndrome. It would be useful to know if this patient has since developed additional autoimmune disorders. Two participant exomes did not contain variations that were included in this study: one was a participant with multiple autoimmune syndrome and one was a participant with Sjogren’s syndrome.
Are the variants meaningful?

MACF1 and KIAA0754
The authors note that the MACF1 gene is a large gene spanning 92 exons. The gene’s size “increases the likelihood of identifying more than one heterozygote in a particular individual by chance (compared to smaller genes), regardless of whether these variants are causative or not.” This directly relates to the participant above who displayed two heterozygous variants in these two genes, one new and one rare. No other study participants shared these variants. Variants in the MACF1/KIAA0754 genes may create risk for metabolic syndrome, but increased risk for autoimmune disorders is not known. The authors did not consider the variants in these genes to be the best candidates for further study, but they did not want to rule out the possibility that they may contribute to autoimmune disease.
(Johar et. al, June 2015)
LRP1 and STAT6
The authors review the “intriguing evidence” they found that the variant in the gene LRP1/STAT6 has the potential to cause multiple autoimmune syndrome. “Intriguing” is about the closest a scientist can come to breathlessly excited.
Networks, pathways, and interaction analyses showed that LRP1 is functionally related to the HLA-B and IL10 genes and it has a substantial impact within immunological pathways and/or reaction to bacterial and other foreign proteins…Indeed, several lines of evidence suggest that LRP1 product is involved in crucial extracellular and intracellular anti-inflammatory pathways that play key roles in maintaining the homeostasis of the immune system [25–29]. Therefore, a damaging mutation in this gene might largely contribute to the occurrence of MAS.
The LRP1 gene is expressed in cells with the job of clearing other cells away. Examples of these kinds of cells are macrophages (translation: big eaters) and brain microglia (translation: small glue), that engulf cellular debris, like cells that have undergone apoptosis (A-pop-toe-sus). Apoptosis is a fun word to say—but it means cells that are dying or have died. Reduced clearance of dying cells by big eating macrophages causes accumulation of cell parts in tissues. This accumulation of debris in tissues causes dendritic cells, which are professional antigen presenting cells that activate naive T-cells, to clear away apoptotic debris. Then, dendritic cells may present self-antigens to naive T cells and activate them into auto reactive T cells. In this way, impaired LRP1 cleaning action by macrophages and brain microglia could cause autoimmunity.
To anthropomorphize cells: it would be like macrophage cells and brain microglia went on a long break and dendritic cells are still busily working away in the tissues to find foreign molecules to present to T cells for destruction, and they simply can’t stand, or navigate through, the accumulating mess. Instead of doing their own job, dendritic cells step in and start cleaning up, but when they’re done, suddenly realize they have to get back to their normal job. Except the mix up in jobs means the dendritic cells weren’t practicing their usual discernment in finding antigens. So, instead of presenting foreign molecules, they’re presenting self-molecules to T cells to train T cells to attack self molecules.
LRP1 has three other known immune functions. 1. Components of LRP1 have been shown to enhance survival during sepsis (systemic infection with organ failure). 2. Inflammatory challenges increase the action of LRP1 in order to limit cascading inflammatory reactions and increase the action of macrophages removing apoptotic cells. 3. LRP1 works inside cells to limit inflammatory processes.
Interleukin 10 and LRP1 are related, and interleukin 10 tamps down the inflammatory response. A mutation that disrupts LRP1’s function
would lead to a hyper inflammatory response, which might account for the elevated IL-10 levels in RA [33] and SS [34].
The authors note that STAT6 is already known to be associated with autoimmunity.
(Johar et. al, June 2015)

MICAL1
The authors consider a variation in this gene to be a good candidate for relevance to autoimmune disorders because it is close to another gene—PTPN22—that is known to be an autoimmune gene. PTPN22 alters the responsiveness of T and B cells (types of white blood cells) associated with some autoimmune diseases, including Sjogren’s syndrome.
(Johar et. al, June 2015)

ICA1
This gene is known to be associated with autoimmunity. “ICA1 interacts with AIRE in the production of self-antigen [37] and therefore has been functionally linked with” Sjogren’s syndrome (SS). This gene also “codes” for another gene—ICA69—which is an auto antigen gene associated with Type 1 diabetes and Sjogren’s syndrome. The authors speculate that gene ICA69—unchecked by a mutated, less functional gene ICA1—can lead to auto reactive T cells attacking organs. ICA69 is particularly expressed in the thyroid, the salivary glands, the brain, and the stomach. “ICA69 autoantibodies have been reported in SS and may reflect the broad spectrum of autoimmune abnormalities in this condition.”
(Johar et. al, June 2015)
DUSP12, GRIN3B, BABAM1, ANKLE1, TMEM161A, FKRP and CELA1
The variations found in these genes did not make it into the discussion section of the study. I am so curious to learn more about the variations shared by study participants on genes DUSP12, TMEM161A and FKRP.
How does this study help me get an accurate diagnosis soon?
This study is exciting, but unfortunately it’s not diagnostic-tool-available-soon exciting. The authors note that their results need to be validated in familial studies in people with multiple autoimmune syndrome. This leads me back to the pressing need for research and research subjects with what has been characterized, probably mischaracterized, as a particularly rare disease: multiple autoimmune syndrome. This study is encouraging because it’s a cost-effective laboratory test that is not particularly painful or invasive—blood draw or cheek swab.
It’s also just one piece of the puzzle. Let’s say one or more of these variants can be proven to be associated with multiple autoimmune syndrome. Alone, it isn’t diagnostic, but as another piece of the puzzle, it has the potential to be a powerful tool in the diagnostic toolbox. Variants known to be associated with multiple autoimmune syndrome could provide the basis for testing drugs targeting the specific process that’s causing symptoms. For instance, a drug designed to boost the cleaning action of the LRP1 gene could be developed for use. I can’t wait to see if Johar et. al and Anaya have published on familial genetic testing in the intervening 7 years.
References
Johar AS, Anaya JM, Andrews D, Patel HR, Field M, Goodnow C, Arcos-Burgos M. Candidate gene discovery in autoimmunity by using extreme phenotypes, next generation sequencing and whole exome capture. Autoimmun Rev. 2015 Mar;14(3):204-9. doi: 10.1016/j.autrev.2014.10.021. Epub 2014 Nov 1. PMID: 25447288.
Johar AS, Mastronardi C, Rojas-Villarraga A, Patel HR, Chuah A, Peng K, Higgins A, Milburn P, Palmer S, Silva-Lara MF, Velez JI, Andrews D, Field M, Huttley G, Goodnow C, Anaya JM, Arcos-Burgos M. Novel and rare functional genomic variants in multiple autoimmune syndrome and Sjögren's syndrome. J Transl Med. 2015 Jun 2;13:173. doi: 10.1186/s12967-015-0525-x. PMID: 26031516; PMCID: PMC4450850.
Whole exome sequencing. National Cancer Institute, National Institutes of Health. (2022). Retrieved December 2, 2022, from https://www.cancer.gov/publications/dictionaries/genetics-dictionary/def/whole-exome-sequencing