


Juvenile idiopathic arthritis is on the cusp of a radical, evidence-based revision.


The past five years of research on Juvenile idiopathic arthritis is robust, and a little overwhelming. You can see from the PubMed search results chart above that since the development of the 2001 classification criteria for Juvenile idiopathic arthritis by the International League of Associations for Rheumatology, research has steadily increased for the last 20 years, and jumped significantly in the last two years. That’s the power of even a flawed study classification criteria. And let’s be real, any classification criteria, no matter how evidence-based, will have its flaws and trade-offs.
Two weeks ago, I had a basic nurse’s knowledge of Juvenile idiopathic arthritis, which frankly, isn’t saying much. Because of the scope of the research, I’ve mostly been haunting summary review articles, like this one, which has a spectacular set of organizational charts, comprehensive medication information and an inflammatory joint illustration I’ll briefly touch on below. I wanted to own this fact, because it’s considered more rigorous to go right to the source to read and evaluate each individual study yourself for evidence quality. With over 1,700 results on Juvenile idiopathic arthritis in the last five years, and my particular constraints, comprehensive and direct source review simply isn’t possible.
I cannot claim that the Diagnosis Description I have created for Juvenile idiopathic arthritis/Adult-onset Still’s disease is as comprehensive as it should be, or even as comprehensive as I would like it to be, but it is a repository of evidence-based information that represents what I am always searching for—and frequently can’t find—when looking for information about a particular autoimmune disease. Is there a type of information you’re searching for, but can’t find? Let me know, and I’ll see what I can find.
Radical Transformation
What’s clear from the research is that Juvenile idiopathic arthritis is on the cusp of a radical, evidence-based revision that is likely to include specific antibody requirements, and rely more on cytokine (immune system proteins that have a pro- or anti-inflammatory effect) and genetic markers. There have been recent, promising breakthroughs in understanding how Juvenile idiopathic arthritis progresses—for all the different sub-types.
In 2019 the Pediatric Rheumatology International Trials Organization embarked on a process to revise its study classification criteria to make it more evidence-based. Their preliminary consensus criteria eliminated the oligoarthritis and polyarthritis sub-types, which are based on the number of joints affected at the onset of disease, greatly simplifying the criteria. Simplified from six sub-types down to four, the new preliminary criteria lists adult equivalents of disease, which could help direct pediatric medication trials, especially if medications already have proven efficacy in the adult form of the disease. This criteria may also prove to be more usefully inclusive, as opposed to erroneously exclusionary, which the International League of Associations for Rheumatology criteria was found to be. The new preliminary criteria appear below.


(Zaripova et. al, 2021)
It’s unclear to me how the psoriatic sub-type is captured in the preliminary criteria, but it’s possible the age differentiation is sufficient based on what is now known about psoriatic Idiopathic juvenile arthritis.
Clinical Limitations
Research is exciting, it’s transformational. But is it translatable to on-the-ground, day-to-day clinical work? In 2019 the American College of Rheumatology reviewed the available scientific evidence to try to assist clinicians with general medication recommendations for Polyarthritis Juvenile idiopathic arthritis. You can see from the chart below that although they made recommendations, the quality of the evidence those recommendations rely on is overall quite low.
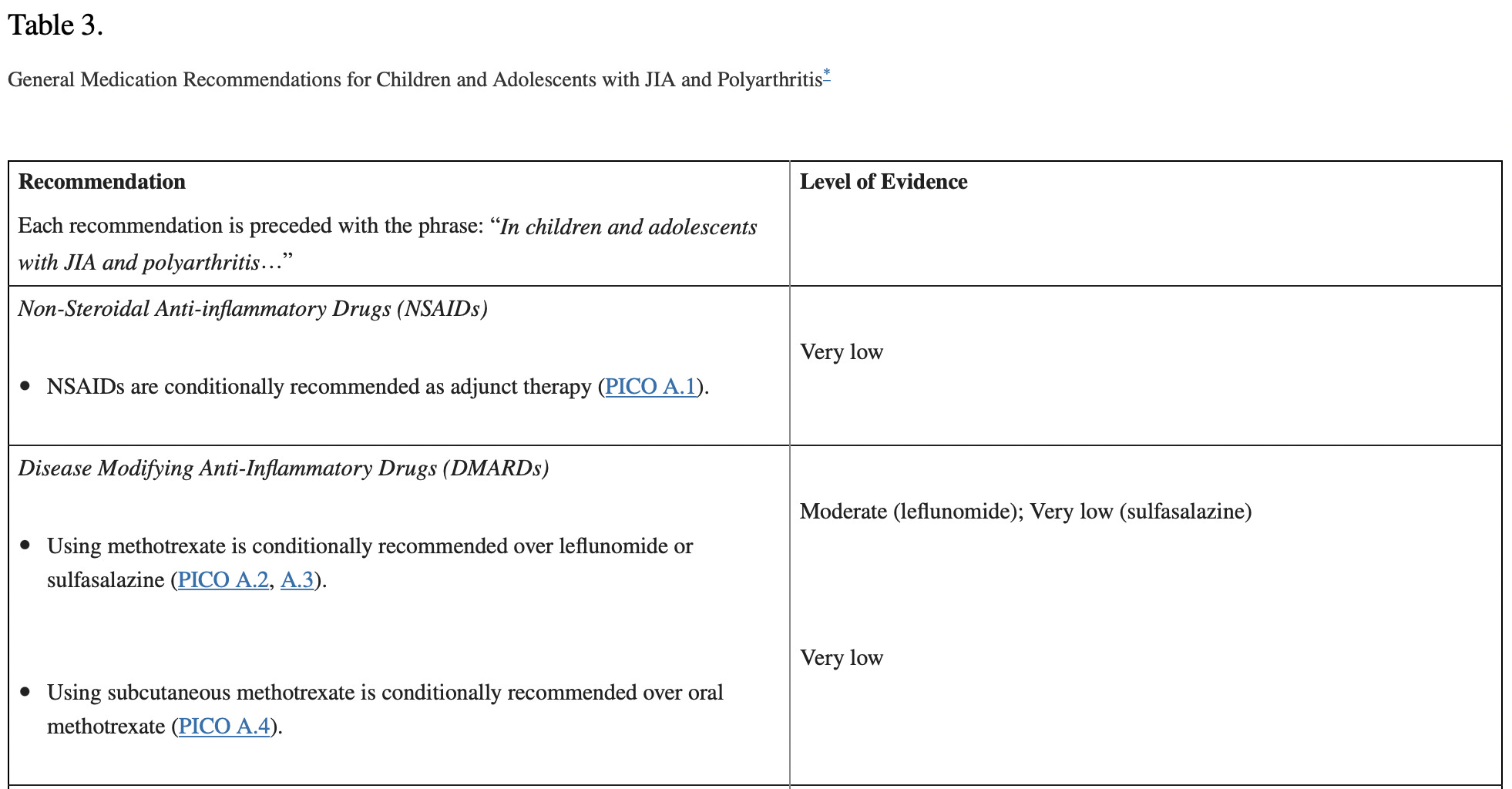


The American College of Rheumatology did note in their medication recommendations: “Importantly, studies in pediatrics are underway or planned for a number of new medications, including Janus kinase inhibitors and interleukin-17 and interleukin-12/23 inhibitors.” There is some hope that new medication recommendations for more targeted therapy will be coming soon from the American College of Rheumatology. It will be interesting to see how they judge the quality of the evidence for the more targeted therapies. The authors do note that recommendations should be used as flexibly as possible “As the quality of evidence was overall low and most recommendations were conditional, clinicians, caregivers, and patients should use a shared decision-making process in considering these recommendations. While these recommendations are intended to address common clinical situations, all treatment decisions must be individualized, with consideration of the unique aspects of each patient’s presentation, medical history, and preferences.” (Ringold et. al, 2019)
I include additional treatment information and algorithms for as many of the sub-types I could find in the Diagnosis Description here.
A Clear Illustration of Autoimmune Joint Inflammation

(Zaripova et. al, 2021)
The illustration above left me wondering how enthesitis-related joint inflammation (inflammation where a tendon or ligament meets bone) compares to this more general illustration of synovial joint inflammation. In other words, what’s the underlying difference between the two? Unfortunately, I couldn’t find an explanatory graphic for enthesitis-related joint inflammation.
I was especially struck, in this illustration, by the “rapid pathological angiogenesis.” Or in plain language, the fast development of new blood vessels, that is both created by the disease process, and serves to multiply the delivery of tissue-destroying immune components, making joint destruction exponentially worse. So many questions popped into my mind, including whether these newly created blood vessels disappear during times when disease is under control, or do they lurk in the joint unused until the next flare, when they become a highway system for haywire autoimmunity again? Is there a limit to the angiogenesis, a kind of joint carrying capacity for newly-created blood vessels? Or do new blood vessels also increase exponentially?
Why It Matters
If you’re diagnosed with Juvenile idiopathic arthritis, particularly, it’s pretty clear how this information could affect you. The way physicians talk to you about your disease may change, the terms they use to describe your diagnosis may change, and the availability of more targeted treatments for your particular disease type may soon be changing. And if you don’t experience those changes in how you interact with your healthcare team, you have more information to ask questions.
For readers who don’t have Juvenile idiopathic arthritis, all research into any autoimmune disease is potentially relevant to your disease process. This is especially true if your disease process is rare and under-studied. Your disease process may have similar immune function problems to this one, it could have similar treatments, and it could be associated with similar genetic profiles.
References
Ringold S, Angeles-Han ST, Beukelman T, Lovell D, Cuello CA, Becker ML, Colbert RA, Feldman BM, Ferguson PJ, Gewanter H, Guzman J, Horonjeff J, Nigrovic PA, Ombrello MJ, Passo MH, Stoll ML, Rabinovich CE, Schneider R, Halyabar O, Hays K, Shah AA, Sullivan N, Szymanski AM, Turgunbaev M, Turner A, Reston J. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Treatment of Juvenile Idiopathic Arthritis: Therapeutic Approaches for Non-Systemic Polyarthritis, Sacroiliitis, and Enthesitis. Arthritis Care Res (Hoboken). 2019 Jun;71(6):717-734. doi: 10.1002/acr.23870. Epub 2019 Apr 25. PMID: 31021516; PMCID: PMC6561125.
Zaripova LN, Midgley A, Christmas SE, Beresford MW, Baildam EM, Oldershaw RA. Juvenile idiopathic arthritis: from aetiopathogenesis to therapeutic approaches. Pediatr Rheumatol Online J. 2021 Aug 23;19(1):135. doi: 10.1186/s12969-021-00629-8. PMID: 34425842; PMCID: PMC8383464.
Thank you for pulling this together. Even as a non-medical professional I could understand much of it.
My son is currently undergoing rheumatological testing (once again). My rheumatologist, my son's dentist and I all suspect Sjogren's (which I also have). However, the rheumatologist wasn't comfortable running the sjogren's specific tests because:
1) initial antibody screens come back negative,
2) until recently he had many other inflammatory sympotms but not persistent joint pain,
3) she says sjogren's in children is highly unlikely (though I am skeptiical on this point)
Recently the joint pain has become persistent - in a presentation similar to that described in the chart as "Polyarticular JIA RF." Food for thought as JIA runs in our family and I have both rheumatoid and psoriatic arthritis as well
I don't know if this round of tests will uncover anything. But I appreciate you covering this topic and pointing us to more recent studies. Undoubtedly this helps me navigate the upcoming medical dicussions in a more informed way. Thank you.