


Eosinophilic fasciitis

Summary
There is a scientific debate about whether Eosinophilic fasciitis is a severe form of Morphea, which is a sub-type of Localized scleroderma. More information about Localized scleroderma and Systemic sclerosis can be found in the Diagnosis Description for Scleroderma found here.
Eosinophilic fasciitis is a very rare condition in which muscle tissue underneath the skin, called fascia, becomes swollen and thick. Rapid swelling can occur in the hands, arms, legs, and feet. People with this condition have a buildup of eosinophils, a type of white blood cell, in the affected fascia and muscles. The exact cause of this condition is unknown. Corticosteroids and other immune-suppressing medications are used to relieve the symptoms. Eosinophilic fasciitis is similar in appearance to scleroderma. However, in contrast with systemic sclerosis, internal organ involvement in Eosinophilic fasciitis is generally absent.
(Genetic and Rare Diseases Information Center, 2023)
Inflammation of the fascia (the tough band of tissue under the skin) along the arms and legs due to abnormal accumulation of white blood cells which causes skin swelling, thickening, and hardening. The symptoms typically impact both sides of the body but have also been seen to only impact one side.
(Global Autoimmune Institute, 2023)
Symptoms
Pain, swelling, inflammation of the skin (particularly on the arms and legs), venous grooving, reddening of the skin, limited mobility of affected areas, thickening/hardening of the skin, joints stuck in unnatural positions, localized areas of scleroderma, fatigue, weight loss, fever, malaise, weakness, muscle pain, joint pain, and bone pain.
(Global Autoimmune Institute, 2023)
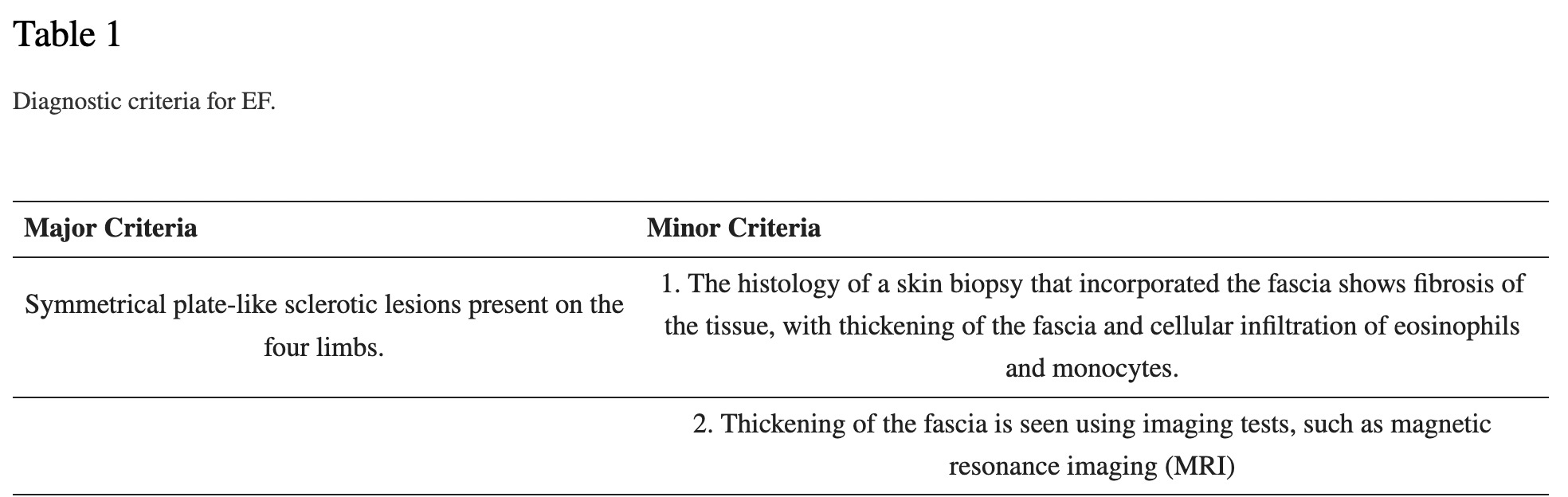
Diagnostic Criteria
The following diagnostic criteria was proposed in 2018 and remains scientifically unvalidated. It requires that the major criterion be met, along with one minor criteria. Raynaud’s phenomenon and Systemic sclerosis are considered exclusion criteria. That is, if either Raynaud’s or Systemic sclerosis are present, then Eosinophilic fasciitis is ruled out. (Jinnin et. al, 2018)
Study Classification Criteria
Variable.
Example: “biopsy-confirmed” Eosinophilic fasciitis, with no further details on the specific tissue pathology criteria used.
Example: retrospective study using diagnostic codes and the search term fasciitis. This is not a rigorous, or well-tested, classification process, and could lead to large variations in study population.
Diagnostic Tests
Full-thickness biopsy, containing fascia and muscle, is the gold standard diagnostic tool. Scant eosinophils may be present, though eosinophils could also be absent in some patients (most diagnostic)
MRI (used mainly when the biopsy is inconclusive, or cannot be performed)
“inflammation on MRI is confirmed by the increased T2 signal in the subcutaneous and deep fascia and the enhancement of the structures on fat-suppressed T1 images after gadolinium administration {contrast solution used in MRI}”
Blood Tests
Complete blood count may show elevated or slightly elevated eosinophils (type of white blood cell: normal levels are 1-3% of the total white blood cells found in a blood sample)
Estimated sedimentation rate (ESR) (general inflammatory marker that is not specifically diagnostic)
C-reactive protein (CRP) (general inflammatory marker that is not specifically diagnostic)
“We observed elevated serum aldolase levels in 3 patients with EF. Serum creatinine kinase levels were within the normal range. We measured the aldolase levels longitudinally. In all patients, the levels decreased to the normal range after oral corticosteroid treatment, and skin sclerosis improved. Afterwards, serum aldolase levels increased again, with the recurrence of skin sclerosis. These observations suggest that serum aldolase level may be a useful indicator of disease activity.” (Fujimoto et. al, 1995)
“The degree of activity of the disease can be appreciated by the increased values of…serum type III procollagen peptide (PIIIP), a marker that reflects disease activity {collagen turnover in the body} and may be useful for monitoring.” I was not able to access the original 2003 study supporting this quote, so I cannot report study size or design.
(Mazilu et. al, 2023)
Organized Autoimmunity
(Alternative Autoimmune Disease Classification: FIEM, MIEM or BIEM, or FEM, MEM or BEM)
sex predominance (is an autoimmune disease primarily found in genetic Females, Males, or equally in Both?)
Unknown (Mertens et. al, 2017)
One study of 34 participants with Eosinophilic fasciitis: 20 female (59%), 14 male (Lebeaux et. al, 2012).
One study of 63 participants with Eosinophilic fasciitis: 43 female (68%), 20 (32%) male (Wright et. al, 2016).
One study of 10 participants with Eosinophilic fasciitis: 6 female, 4 male (Tull et. al, 2018)
One study of 78 participants with Eosinophilic fasciitis: 47 female (60%), 31 male (40%) (Li et. al, 2020)
One study of 45 participants with Eosinophilic fasciitis: 35 male (77.8%), 10 female (Yang et. al, 2023)
One study of 89 participants with Eosinophilic fasciitis had a female to male ratio of 1:1 (Mango et. al, 2020)
Inherited and acquired gene variations that cause increased susceptibility
Human Leukocyte Antigen (HLA) Associations
Not specifically studied in patients with Eosinophilic fasciitis. Eosinophilic fasciitis may be a sub-type of Localized scleroderma (also known as Morphea). More information about HLA associations to Localized scleroderma can be found in the diagnosis description for Scleroderma here.
Other Gene Variations (mutations)
Unstudied, at this time.
Gene Triggering Environmental Exposures
Infections
Borrelia burgdorferi, better known as the Lyme disease spirochete (Granter et. al, 1996). The case series cited includes four patients with spirochete identification, two with a definitive identification of Borrelia burgdorferi.
Drugs
Check Point Inhibitors, a class of relatively new cancer treatment drugs. The following drugs in this class have been implicated in the development of Eosinophilic fasciitis:
Nivolumab (Le Tallec et. al, 2020 and Chan et. al, 2020 and Teboul et. al, 2022)
atezolizumab (Chan et. al, 2020)
pembrolizumab (Chan et. al, 2020 and Zampeli et. al, 2021)
Statins, a well-known class of drugs used to treat increased levels of cholesterol. This study used an international drug adverse reaction reporting database (Vigibase) to conduct their study. Due to its retrospective, observational design, I’m only listing the drugs with more than one adverse reaction reported.
Fluvastatin (Teboul et. al, 2022)
Atorvastatin (Teboul et. al, 2022)
Toxins
1980s outbreak of Eosinophilic fasciitis in Spain due to adulterated rapeseed oil (Mazilu et. al, 2023)
Stress
Strenuous exercise was associated with 46% and 28% of Eosinophilic fasciitis cases in two case series (Mertens et. al, 2017)
Needs to be assessed for each patient
Multiple interactive and destructive immune system pathologies
Moy et. al compared the tissue pathology of 12 participants with Localized scleroderma (morphea) to 8 participants with Eosinophilic fasciitis. They found that the T Helper 1 (Th1) and T Helper 2 (Th2) cells were significantly lower in Localized scleroderma compared to Eosinophilic fasciitis. T Helper 17 (Th17) cells were significantly higher in Eosinophilic fasciitis. This finding could help to differentiate between these conditions. (Moy et. al, 2017)
For more explanation on T Helper cells: “Effector Th1 cells produce proinflammatory cytokines such as INF-γ and lymphotoxin-α. These cytokines organize inflammatory centers and enhance cellular immune response; moreover, intracellular pathogens such as Mycobacteria and Salmonella spp, and other intravesicular agents are killed by IFN-γ through the activation of antimicrobial defenses. Th1 cytokine production is also characteristic of many organ-specific autoimmune diseases, including rheumatoid arthritis, insulin-dependent diabetes mellitus, experimental autoimmune encephalitis, and others. Effector Th2 cells, in contrast, produce a different profile of cytokines (IL-4, IL-5, IL-9, IL-10, IL-13, and so on) that together instruct B cells to proliferate and differentiate into antibody-secreting plasma cells, and potentiate the function of several cell types in antiparasite responses. As such, Th2 cells play an important role in providing protection against certain extracellular pathogens, such as bacteria and a variety of parasites, and are also involved in asthmatic reactions.” (Dong & Flavell, 2000)
Tissue-Type or Cell-Type Attacked
Theories of how the tissues are affected in Eosinophilic fasciitis are based on scientific evidence of disease causing mechanisms in Localized scleroderma and Systemic sclerosis. Just to be clear, the following theory has not been specifically studied in participants with Eosinophilic fasciitis. For Eosinophilic fasciitis, it may be less about what is destroyed, and more about what is preserved and caused to proliferate. The development of excessive collagen synthesis, along with signals to decrease collagen breakdown in the deep tissues may be the cause of fibrosis in Eosinophilic fasciitis. It’s still unknown what the underlying cause of fibrosis is in Localized scleroderma and Systemic sclerosis. (Mertens et. al, 2017)
What is “Fascia?”
Fascia was always a vague concept to me—sort of a connective tissue catch all whose location in the body I could never quite pin down. Turns out, the basis for my confusion is systemic:
Researchers do not agree on one comprehensive "fascia" definition. Despite the scientific uncertainty, there is an agreement with medical text that the fascia covers every structure of the body, creating a structural continuity that gives form and function to every tissue and organ. The fascial tissue has a ubiquitous distribution in the body system; it is able to wrap, interpenetrate, support, and form the bloodstream, bone tissue, meningeal tissue, organs, and skeletal muscles. The fascia creates different interdependent layers with several depths, from the skin to the periosteum {tissue surrounding bone}, forming a three-dimensional mechano-metabolic structure.
(Bordoni et. al, 2022)
There are four organizations that have published four different definitions of “fascia” that you can read more about here. In the context of Eosinophilic fasciitis, it might be most useful to consider the oldest definition of “fascia,” which excludes the epidermis, or the topmost portion of the skin. So, inflammation that extends deeper into the tissues underlying the epidermis could be characterized as “fasciitis.”
Treatment(s)
The therapeutic approach in EF is currently unclear; there are also no randomized studies regarding therapy in EF.
(Mazilu et. al, 2023)
Mertens et. al attempts to create a proposed treatment algorithm that slightly elevates Methotrexate over systemic Corticosteroids (abbreviated MTX and SCS, respectively, in the flow chart below) for the treatment of Eosinophilic fasciitis:


After following up over 3 years later, Wright et. al (2016), found that “complete response was more likely with the combination of corticosteroids and methotrexate (21 of 33 patients [64%]) compared with other treatment combinations.” They define complete response as “resolution of erythema and/or edema with no or minimal persistent induration {hardening}.” Their study was an observational cross-sectional design, which is the weakest type of observational study. By weak, I mean the most susceptible to hidden bias that could influence the results.
For more information on treatment, please see a post I wrote titled Eosinophilic fasciitis: Evidence for Treatment and Response.
Managing Specialist(s)
Dermatologist
Rheumatologist
Research Authors
Canada
Asfandyar Mufti, MD, Division of Dermatology, University of Toronto, Toronto, Canada
Jensen Yeung, MD, Division of Dermatology, Women's College Hospital, Toronto, Canada
China
Yun Li, Department of Dermatology, Beijing Tian Tan Hospital, Capital Medical University, Beijing, China and Department of Dermatology, Chinese Academy of Medical Sciences, Peking Union Medical College, Peking Union Medical College Hospital, Beijing, China
Xing Chang, Department of Education, Chinese Academy of Medical Sciences, Peking Union Medical College, Peking Union Medical College Hospital, Beijing, China
Wei Du, Department of Dermatology, Chinese Academy of Medical Sciences, Peking Union Medical College, Peking Union Medical College Hospital, Beijing, China
Yue-Ping Zeng, Department of Dermatology, Chinese Academy of Medical Sciences, Peking Union Medical College, Peking Union Medical College Hospital, Beijing, China
Xie Yuan, Department of Dermatology, Chinese Academy of Medical Sciences, Peking Union Medical College, Peking Union Medical College Hospital, Beijing, China
Jun Li, Department of Dermatology, Beijing Tian Tan Hospital, Capital Medical University, Beijing, China
Li Jia, Department of Dermatology, Chinese Academy of Medical Sciences, Peking Union Medical College, Peking Union Medical College Hospital, Beijing, China
Tao Zhang, Department of Dermatology, Chinese Academy of Medical Sciences, Peking Union Medical College, Peking Union Medical College Hospital, Beijing, China
Yong Xie, Department of Dermatology, Chinese Academy of Medical Sciences, Peking Union Medical College, Peking Union Medical College Hospital, Beijing, China
Qing Li, Department of Dermatology, Beijing Tian Tan Hospital, Capital Medical University, Beijing, China
Qiu-Ning Sun, Department of Dermatology, Chinese Academy of Medical Sciences, Peking Union Medical College, Peking Union Medical College Hospital, Beijing, China
Japan
Masatoshi Jinnin, M.D., Ph.D., Department of Dermatology and Plastic Surgery, Faculty of Life Sciences, Kumamoto University, Honjo, Kumamoto, Japan
Toshiyuki Yamamoto, Department of Dermatology, School of Medicine, Fukushima Medical University, Fukushima, Japan
Yoshihide Asano, Department of Dermatology, The University of Tokyo Hospital, Tokyo, Japan
Osamu Ishikawa, Department of Dermatology, Graduate School of Medicine, Gunma University, Gunma, Japan
Shinichi Sato, Department of Dermatology, The University of Tokyo Hospital, Tokyo, Japan
Kazuhiko Takehara, Department of Molecular Pathology of Skin, Faculty of Medicine, Institute of Medical, Pharmaceutical and Health Sciences, Kanazawa University, Kanazawa, Japan
Minoru Hasegawa, Department of Dermatology Division, Division of Medicine, Faculty of Medical Sciences, University of Fukui, Fukui, Japan
Manabu Fujimoto, Department of Dermatology, Faculty of Medicine, University of Tsukuba, Tsukuba, Japan
Hironobu Ihn, Department of Dermatology and Plastic Surgery, Faculty of Life Sciences, Kumamoto University, Kumamoto, Japan
Romania
Diana Mazilu, “Sfanta Maria” Clinical Hospital, Bucharest, Romania and “Carol Davila” University of Medicine, Bucharest, Romania
Laura Alina Boltașiu (Tătaru), “Sfanta Maria” Clinical Hospital, Bucharest, Romania
Denise-Ani Mardale, “Sfanta Maria” Clinical Hospital, Bucharest, Romania and “Carol Davila” University of Medicine, Bucharest, Romania
Maria Silviana Bijă, “Sfanta Maria” Clinical Hospital, Bucharest, Romania
Sermina Ismail, “Sfanta Maria” Clinical Hospital, Bucharest, Romania
Violeta Zanfir, “Sfanta Maria” Clinical Hospital, Bucharest, Romania
Florentina Negoi, “Sfanta Maria” Clinical Hospital, Bucharest, Romania
Andra Rodica Balanescu, “Sfanta Maria” Clinical Hospital, Bucharest, Romania and “Carol Davila” University of Medicine, Bucharest, Romania
United States
Connecticut
Vaidehi R. Chowdhary, Section of Rheumatology, Allergy and Immunology, Yale University School of Medicine, New Haven, CT, USA
Minnesota
Robert L. Mango, Essentia Health Duluth Clinic, Duluth, MN, USA
Cynthia S. Crowson, Division of Rheumatology, Department of Medicine, Mayo Clinic College of Medicine, Rochester, MN, USA
Lisa A. Drage, Department of Dermatology, Mayo Clinic College of Medicine, Rochester, MN, USA
David A. Wetter, Department of Dermatology, Mayo Clinic College of Medicine, Rochester, MN, USA
Julia S. Lehman, Department of Dermatology, Mayo Clinic College of Medicine, Rochester, MN, USA and Department of Laboratory Medicine and Pathology, Mayo Clinic College of Medicine, Rochester, MN, USA
Margot S. Peters, Department of Dermatology, Mayo Clinic College of Medicine, Rochester, MN, USA and Department of Laboratory Medicine and Pathology, Mayo Clinic College of Medicine, Rochester, MN, USA
Mark D. Davis, Department of Dermatology, Mayo Clinic College of Medicine, Rochester, MN, USA
New York
Karmela Kim Chan, Department of Medicine, Hospital for Special Surgery, New York, New York USA
Cynthia Magro, Department of Pathology and Laboratory Medicine, Weill Cornell Medicine, New York, New York USA
Alexander Shoushtari, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York USA
Charles Rudin, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York USA
Veronica Rotemberg, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York USA
Anthony Rossi, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York USA
Cecilia Lezcano, Department of Pathology, Memorial Sloan Kettering Cancer Center, New York, New York USA
John Carrino, Department of Radiology, Hospital for Special Surgery, New York, New York USA
David Fernandez, Department of Medicine, Hospital for Special Surgery, New York, New York USA
Michael A. Postow, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York USA
Arlyn Apollo, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York USA
Mario E. Lacouture, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York USA
Anne R. Bass, Department of Medicine, Hospital for Special Surgery, New York, New York USA
Ohio
Kubra Bugdayli, MetroHealth Medical Center, Cleveland, OH, USA
Pennsylvania
Xu-Ming Mao, Department of Dermatology, University of Pennsylvania, Philadelphia, PA, USA.
Research Institutions
Canada
University of Toronto, Toronto, Canada
Women's College Hospital, Toronto, Canada
China
Beijing Tian Tan Hospital, Capital Medical University, Beijing, China
Chinese Academy of Medical Sciences, Peking Union Medical College, Peking Union Medical College Hospital, Beijing, China
Japan
Kumamoto University, Honjo, Kumamoto, Japan
Fukushima Medical University, Fukushima, Japan
The University of Tokyo Hospital, Tokyo, Japan
Gunma University, Gunma, Japan
Kanazawa University, Kanazawa, Japan
University of Fukui, Fukui, Japan
University of Tsukuba, Tsukuba, Japan
Romania
“Sfanta Maria” Clinical Hospital, Bucharest, Romania
“Carol Davila” University of Medicine, Bucharest, Romania
United States
Connecticut
Yale University School of Medicine, New Haven, CT, USA
Minnesota
Essentia Health Duluth Clinic, Duluth, MN, USA
Division of Rheumatology, Department of Medicine, Mayo Clinic College of Medicine, Rochester, MN, USA
Department of Dermatology, Mayo Clinic College of Medicine, Rochester, MN, USA
New York
Hospital for Special Surgery, New York, New York USA
Weill Cornell Medicine, New York, New York USA
Memorial Sloan Kettering Cancer Center, New York, New York USA
Pennsylvania
University of Pennsylvania, Philadelphia, PA, USA.
Ohio
MetroHealth Medical Center, Cleveland, OH, USA
Average Time from Symptom Onset to Diagnosis
Approximately 11 months in a retrospective study of 63 participants (Wright et. al, 2016).
Last Updated
August 21, 2023
References
Chan KK, Magro C, Shoushtari A, Rudin C, Rotemberg V, Rossi A, Lezcano C, Carrino J, Fernandez D, Postow MA, Apollo A, Lacouture ME, Bass AR. Eosinophilic Fasciitis Following Checkpoint Inhibitor Therapy: Four Cases and a Review of Literature. Oncologist. 2020 Feb;25(2):140-149. doi: 10.1634/theoncologist.2019-0508. Epub 2019 Oct 15. PMID: 32043775; PMCID: PMC7011633.
Dong, C., Flavell, R.A. Cell fate decision: T-helper 1 and 2 subsets in immune responses. Arthritis Res Ther 2, 179 (2000). https://doi.org/10.1186/ar85
Eosinophilic fasciitis. Global Autoimmune Institute. (2023, February). Retrieved on July 11, 2023 from https://www.autoimmuneinstitute.org/autoimmune-resources/autoimmune-diseases-list/eosinophilic-fasciitis/
Eosinophilic fasciitis. National Institutes of Health, National Center for Advancing Translational Sciences, Genetic and Rare Diseases Information Center. (2023, February). Retrieved on July 11, 2023 from https://rarediseases.info.nih.gov/diseases/6351/eosinophilic-fasciitis
Fujimoto M, Sato S, Ihn H, Kikuchi K, Yamada N, Takehara K. Serum aldolase level is a useful indicator of disease activity in eosinophilic fasciitis. J Rheumatol, 22 (1995), pp. 563-565
Granter SR, Barnhill RL, Duray PH. Borrelial fasciitis: diffuse fasciitis and peripheral eosinophilia associated with Borrelia infection. Am J Dermatopathol. 1996 Oct;18(5):465-73. doi: 10.1097/00000372-199610000-00004. PMID: 8902092.
Jacobe H, Ahn C, Arnett FC, Reveille JD. Major histocompatibility complex class I and class II alleles may confer susceptibility to or protection against morphea: findings from the Morphea in Adults and Children cohort. Arthritis Rheumatol. 2014 Nov;66(11):3170-7. doi: 10.1002/art.38814. Erratum in: Arthritis Rheumatol. 2015 Mar;67(3):751. PMID: 25223600; PMCID: PMC4211936.
Jinnin M, Yamamoto T, Asano Y, Ishikawa O, Sato S, Takehara K, Hasegawa M, Fujimoto M, Ihn H. Diagnostic criteria, severity classification and guidelines of eosinophilic fasciitis. J Dermatol. 2018 Aug;45(8):881-890. doi: 10.1111/1346-8138.14160. Epub 2017 Dec 13. PMID: 29235676.
Lebeaux D, Francès C, Barete S, Wechsler B, Dubourg O, Renoux J, Maisonobe T, Benveniste O, Gatfossé M, Bourgeois P, Amoura Z, Cacoub P, Piette JC, Sène D. Eosinophilic fasciitis (Shulman disease): new insights into the therapeutic management from a series of 34 patients. Rheumatology (Oxford). 2012 Mar;51(3):557-61. doi: 10.1093/rheumatology/ker366. Epub 2011 Nov 25. PMID: 22120602.
Le Tallec E, Lescoat A, Ballerie A, Cador B, Lena H, Ricordel C, Damien S, Lebbe C, Jego P, Belhomme N. Eosinophilic Fasciitis Triggered by Nivolumab: A Remarkable Efficacy of the mTOR Inhibitor Sirolimus. J Thorac Oncol. 2020 Feb;15(2):e29-e30. doi: 10.1016/j.jtho.2019.09.011. PMID: 32127188.
Li Y, Chang X, Mao XM, Du W, Zeng YP, Yuan X, Li J, Jia L, Zhang T, Xie Y, Li Q, Sun QN. Clinical and pathologic features and therapeutic management of eosinophilic fasciitis. Chin Med J (Engl). 2020 Sep 10;134(5):616-618. doi: 10.1097/CM9.0000000000001078. PMID: 32925284; PMCID: PMC7929001.
Mango RL, Bugdayli K, Crowson CS, Drage LA, Wetter DA, Lehman JS, Peters MS, Davis MD, Chowdhary VR. Baseline characteristics and long-term outcomes of eosinophilic fasciitis in 89 patients seen at a single center over 20 years. Int J Rheum Dis. 2020 Feb;23(2):233-239. doi: 10.1111/1756-185X.13770. Epub 2019 Dec 6. PMID: 31811710.
Mazilu D, Boltașiu Tătaru LA, Mardale DA, Bijă MS, Ismail S, Zanfir V, Negoi F, Balanescu AR. Eosinophilic Fasciitis: Current and Remaining Challenges. Int J Mol Sci. 2023 Jan 19;24(3):1982. doi: 10.3390/ijms24031982. PMID: 36768300; PMCID: PMC9916848.
Mertens JS, Seyger MMB, Thurlings RM, Radstake TRDJ, de Jong EMGJ. Morphea and Eosinophilic Fasciitis: An Update. Am J Clin Dermatol. 2017 Aug;18(4):491-512. doi: 10.1007/s40257-017-0269-x. PMID: 28303481; PMCID: PMC5506513.
Moy AP, Maryamchik E, Nikolskaia OV, Nazarian RM. Th1- and Th17-polarized immune infiltrates in eosinophilic fasciitis-A potential marker for histopathologic distinction from morphea. J Cutan Pathol. 2017 Jun;44(6):548-552. doi: 10.1111/cup.12947. PMID: 28393380.
Teboul A, Chouchana L, Durrieu G, Eftekhari P, Treluyer JM, Mouthon L, Chaigne B. Drug-induced eosinophilic fasciitis: A dual pharmacovigilance analysis. J Am Acad Dermatol. 2022 Jun;86(6):1372-1375. doi: 10.1016/j.jaad.2021.05.030. Epub 2021 May 27. PMID: 34052335.
Tull R, Hoover WD 3rd, De Luca JF, Huang WW, Jorizzo JL. Eosinophilic fasciitis: a case series with an emphasis on therapy and induction of remission. Drugs Context. 2018 Oct 2;7:212529. doi: 10.7573/dic.212529. PMID: 30302114; PMCID: PMC6172017.
Wright NA, Mazori DR, Patel M, Merola JF, Femia AN, Vleugels RA. Epidemiology and Treatment of Eosinophilic Fasciitis: An Analysis of 63 Patients From 3 Tertiary Care Centers. JAMA Dermatol. 2016;152(1):97–99. doi:10.1001/jamadermatol.2015.3648
Yang J, Wan Y, Zhang J, Zhu J. [Clinical characteristics, ultrasonic diagnosis, treatment and outcomes of eosinophilic fasciitis: a retrospective single-center analysis of 45 cases]. Nan Fang Yi Ke Da Xue Xue Bao. 2023 Jan 20;43(1):145-152. Chinese. doi: 10.12122/j.issn.1673-4254.2023.01.21. PMID: 36856224; PMCID: PMC9978722.
Zampeli E, Zervas E. Eosinophilic Fasciitis following Checkpoint Inhibitor Therapy with Pembrolizumab. Mediterr J Rheumatol. 2021 Dec 27;32(4):376-377. doi: 10.31138/mjr.32.4.376. PMID: 35128334; PMCID: PMC8802204.